Fill Out Your Wisconsin 812 Template
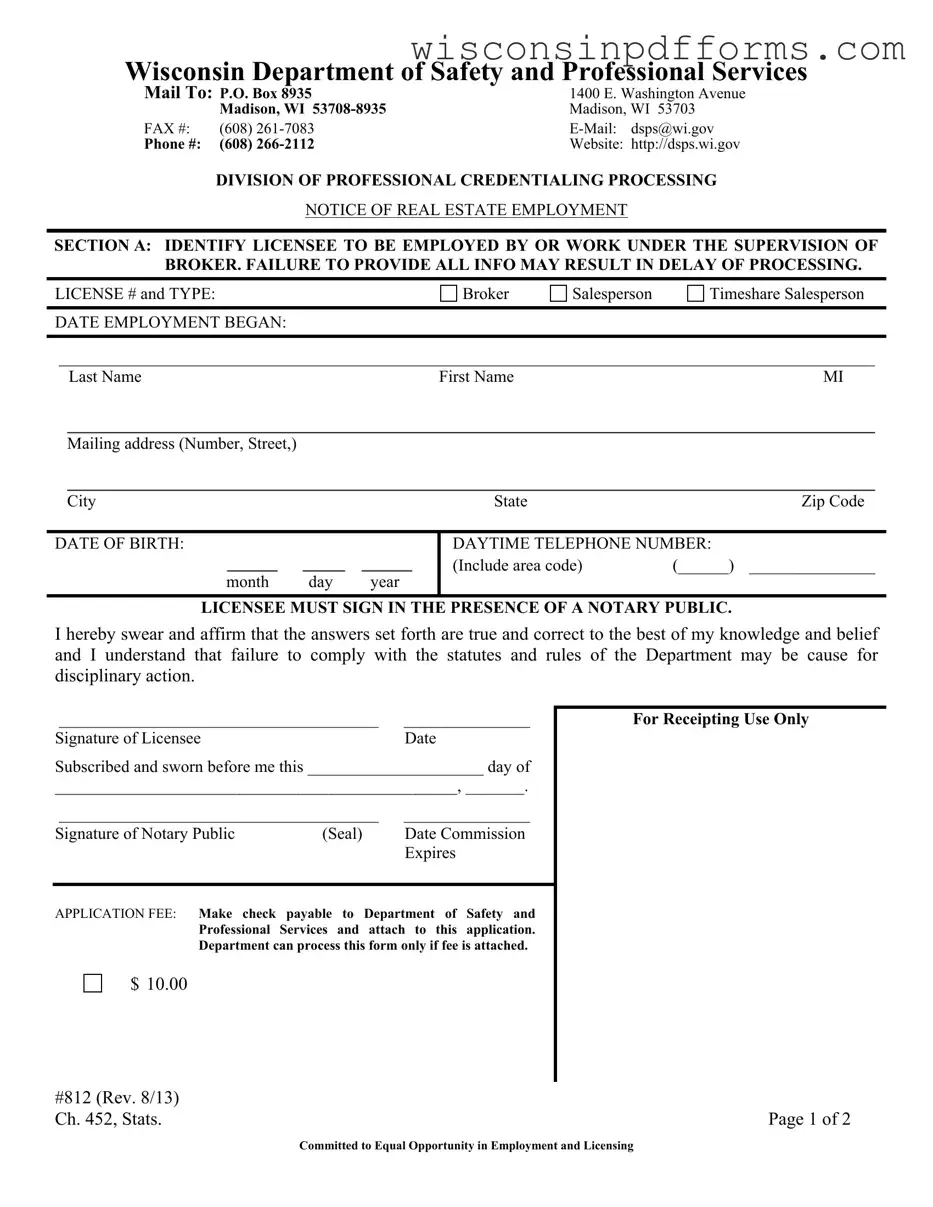
The Wisconsin 812 form is an essential document for real estate professionals in the state, serving as a notice of employment that links licensees with their respective brokers. This form is required by the Wisconsin Department of Safety and Professional Services and must be completed accurately to avoid delays in processing. It includes crucial sections where the licensee identifies themselves, providing details such as their license type—whether they are a broker, salesperson, or timeshare salesperson—and their employment start date. The licensee must also provide personal information, including their mailing address and date of birth, and must sign the form in the presence of a notary public to affirm the accuracy of the information provided. Additionally, the form requires the broker-employer to confirm their responsibility for the licensee, ensuring compliance with state statutes and rules. A nominal application fee must accompany the form, highlighting the importance of timely submission for those looking to establish their professional standing in the real estate market.
Form Example
Wisconsin Department of Safety and Professional Services
Mail To: P.O. Box 8935 |
1400 E. Washington Avenue |
||
|
Madison, WI |
Madison, WI 53703 |
|
FAX #: |
(608) |
dsps@wi.gov |
|
Phone #: |
(608) |
Website: |
http://dsps.wi.gov |
DIVISION OF PROFESSIONAL CREDENTIALING PROCESSING
NOTICE OF REAL ESTATE EMPLOYMENT
SECTION A: IDENTIFY LICENSEE TO BE EMPLOYED BY OR WORK UNDER THE SUPERVISION OF BROKER. FAILURE TO PROVIDE ALL INFO MAY RESULT IN DELAY OF PROCESSING.
LICENSE # and TYPE: |
Broker |
Salesperson |
Timeshare Salesperson |
|
|
|
|
DATE EMPLOYMENT BEGAN: |
|
|
|
|
|
|
|
_________________________________________________________________________________________________
Last NameFirst NameMI
________________________________________________________________________________________________
Mailing address (Number, Street,)
________________________________________________________________________________________________
City |
State |
Zip Code |
DATE OF BIRTH:
______ _____ ______
month day year
DAYTIME TELEPHONE NUMBER:
(Include area code) |
(______) _______________ |
LICENSEE MUST SIGN IN THE PRESENCE OF A NOTARY PUBLIC.
I hereby swear and affirm that the answers set forth are true and correct to the best of my knowledge and belief and I understand that failure to comply with the statutes and rules of the Department may be cause for disciplinary action.
______________________________________ |
_______________ |
Signature of Licensee |
Date |
Subscribed and sworn before me this _____________________ day of
________________________________________________, _______.
______________________________________ |
_______________ |
|
Signature of Notary Public |
(Seal) |
Date Commission |
|
|
Expires |
APPLICATION FEE: Make check payable to Department of Safety and
Professional Services and attach to this application. Department can process this form only if fee is attached.
For Receipting Use Only
$ 10.00
#812 (Rev. 8/13) |
|
Ch. 452, Stats. |
Page 1 of 2 |
Committed to Equal Opportunity in Employment and Licensing
Wisconsin Department of Safety and Professional Services
SECTION B: THIS SECTION IDENTIFIES THE BROKER WITH WHOM OR BY WHOM THE
LICENSEE IN SECTION A WILL BE ASSOCIATED OR EMPLOYED
TYPE OF LICENSE: |
Sole Proprietor Broker
Business Entity (Association, LLC, LLP)
PRINT NAME AND ADDRESS OF
_________________________________________________________________________________________________
Business Entity Name
_________________________________________________________________________________________________
Business Address of
_____________________________________________ |
(_____) ______________________________________ |
License Number: |
Main Office Telephone Number: |
This statement must be signed by the sole proprietor
This is to certify that the
_________________________________________________________
Print name of person signing below |
|
_________________________________________________________ |
________________________ |
Signature of either the sole proprietor broker or a director, manager, |
Date |
member, officer, owner or partner of the licensed business |
|
entity listed above. |
|
|
|
#812 (Rev. 8/13) |
|
Ch. 452, Stats. |
Page 2 of 2 |
Committed to Equal Opportunity in Employment and Licensing
Document Specs
| Fact Name | Description |
|---|---|
| Governing Law | The Wisconsin 812 form is governed by Chapter 452 of the Wisconsin Statutes, which outlines regulations for real estate licenses and employment. |
| Application Fee | To process the Wisconsin 812 form, an application fee of $10.00 must be attached. The fee is payable to the Department of Safety and Professional Services. |
| Notary Requirement | The licensee must sign the form in the presence of a notary public. This signature affirms that the information provided is true and correct. |
| Contact Information | For inquiries, individuals can contact the Department of Safety and Professional Services at (608) 266-2112 or via email at dsps@wi.gov. |
Popular PDF Forms
Wisconsin Doa 3009 - Parents or legal guardians might employ the form to monitor the driving records of their teen drivers, as part of ensuring their safety on the road.
For those seeking to draft a comprehensive and effective document, utilizing resources like PDF Templates Online can streamline the process of creating a well-structured Lease Agreement that meets legal standards and protects the interests of both landlords and tenants.
Check Homestead Status Wisconsin - The form includes provisions for claimants with disabilities and those over 62 without earned income, reflecting the program's inclusivity.
Iris Wisconsin - Key to the document is its focus on maintaining or improving the participant's quality of life through targeted support and services.