Fill Out Your Wisconsin F 62019 Template
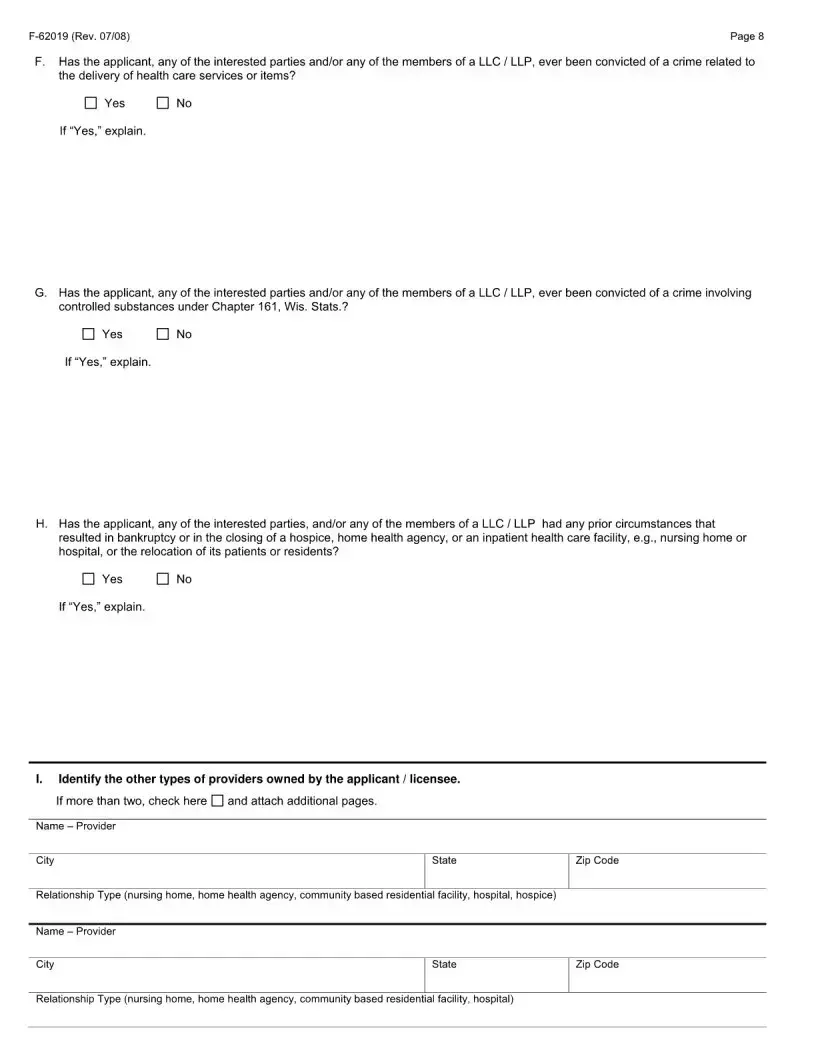
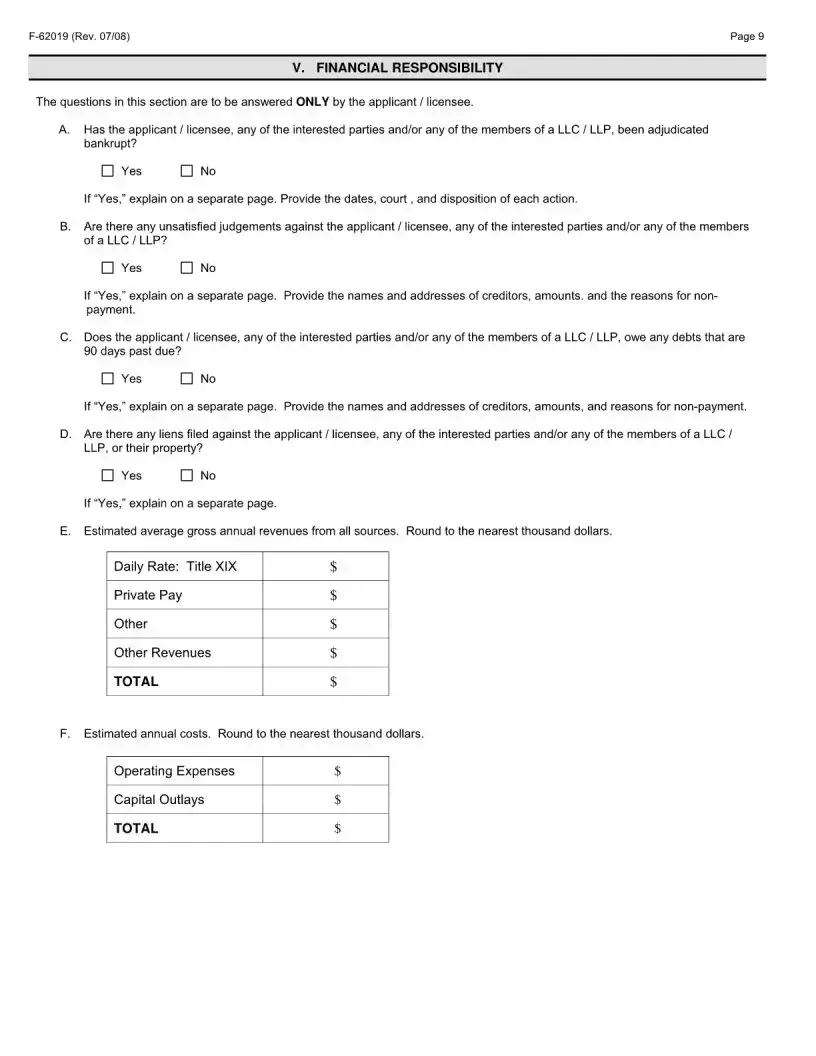
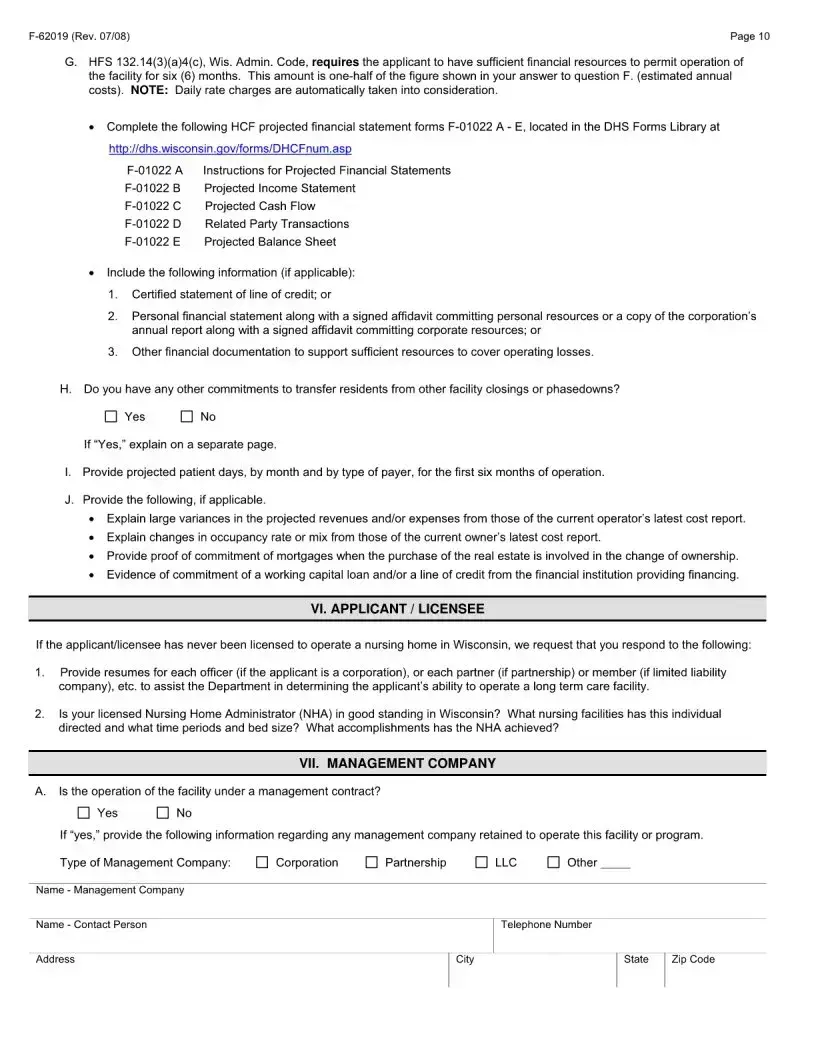
The Wisconsin F-62019 form serves as a crucial document for individuals and organizations seeking to obtain a license for various types of healthcare facilities, including nursing homes, facilities for the developmentally disabled, and institutes for mental disease. This form is designed to gather essential information about the facility, its administration, and ownership structure. Applicants must provide details such as the facility's name, address, and type of care offered, along with the specific license type they are applying for—whether it be for initial licensure, a change of ownership, or a replacement facility. Additionally, the form requires information about the facility's administrator, director of nursing, and medical director, ensuring that qualified personnel are in place to oversee operations. The licensing process is governed by state regulations, which mandate that all requested information be submitted before a license can be issued. This form also collects personally identifiable information, which is strictly used for determining eligibility and statistical purposes. Completing the F-62019 form accurately is a vital step in ensuring compliance with Wisconsin's health and safety standards.
Form Example
Document Specs
| Fact Name | Details |
|---|---|
| Form Purpose | This form is used to apply for a license for nursing homes, facilities for the developmentally disabled, or institutes for mental disease in Wisconsin. |
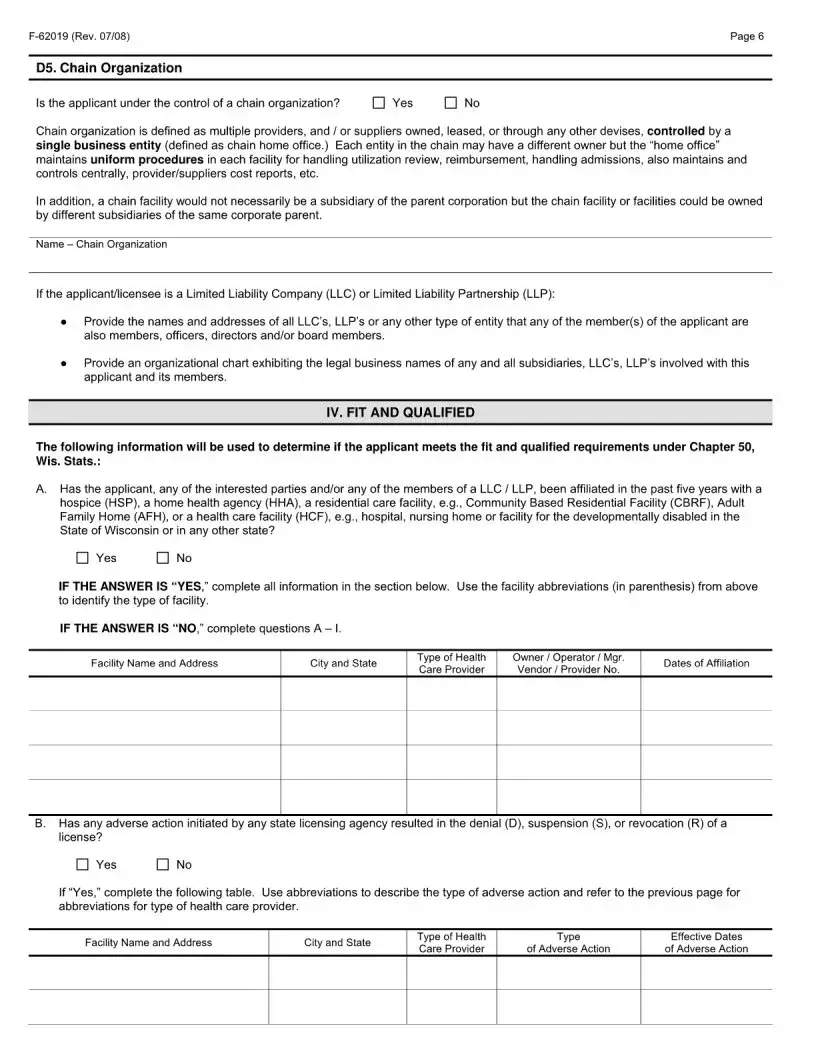
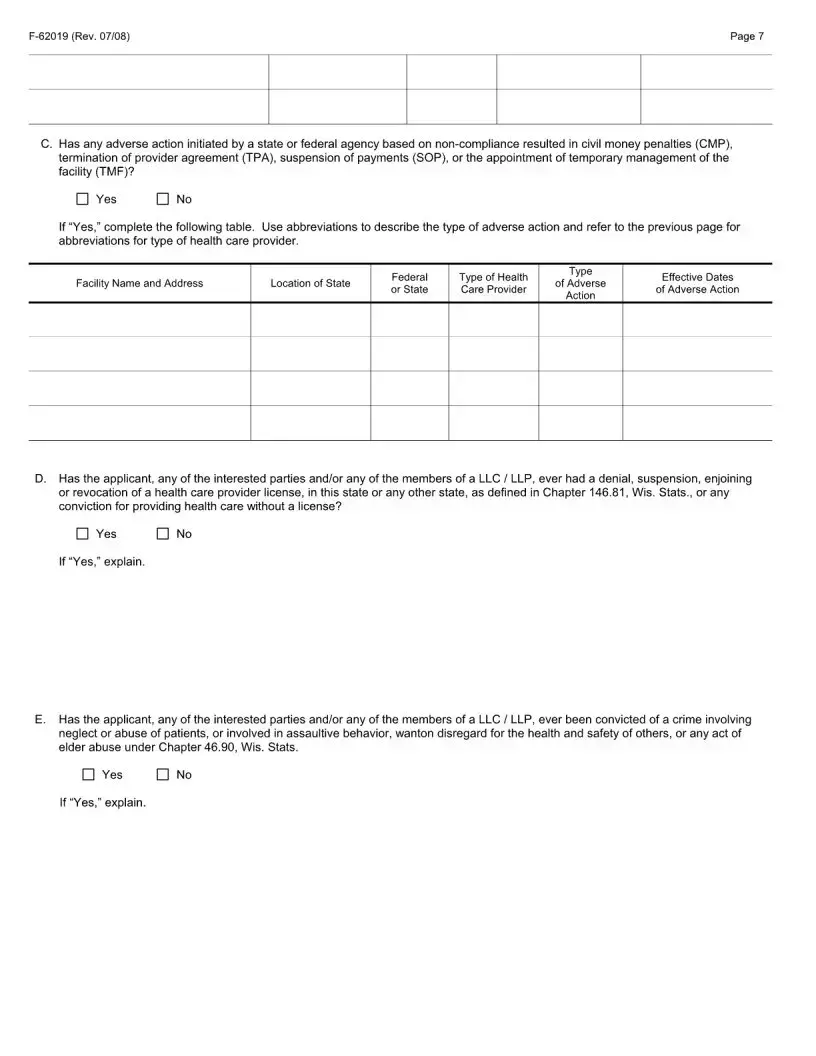
| Governing Laws | The completion of this form is required by Chapter 50.50.03(3)(b) of the Wisconsin Statutes and HFS 132.14(2) and HFS 134.14(1) of the Wisconsin Administrative Code. |
| License Types | Applicants can apply for different types of licenses, including nursing homes, facilities for the developmentally disabled, or institutes for mental disease. |
| Application Types | Applications can be for initial licensing, change of ownership, or replacement facilities. |
| Submission Address | Completed applications should be sent to the Division of Quality Assurance, Bureau of Technology, Licensing and Education, P.O. Box 2969, Madison, WI 53701-2969. |
| Information Use | The personal information collected will only be used to determine licensure eligibility and for statistical purposes. |
| Administrator Information | The form requires details about the facility's administrator, including their status and license number. |
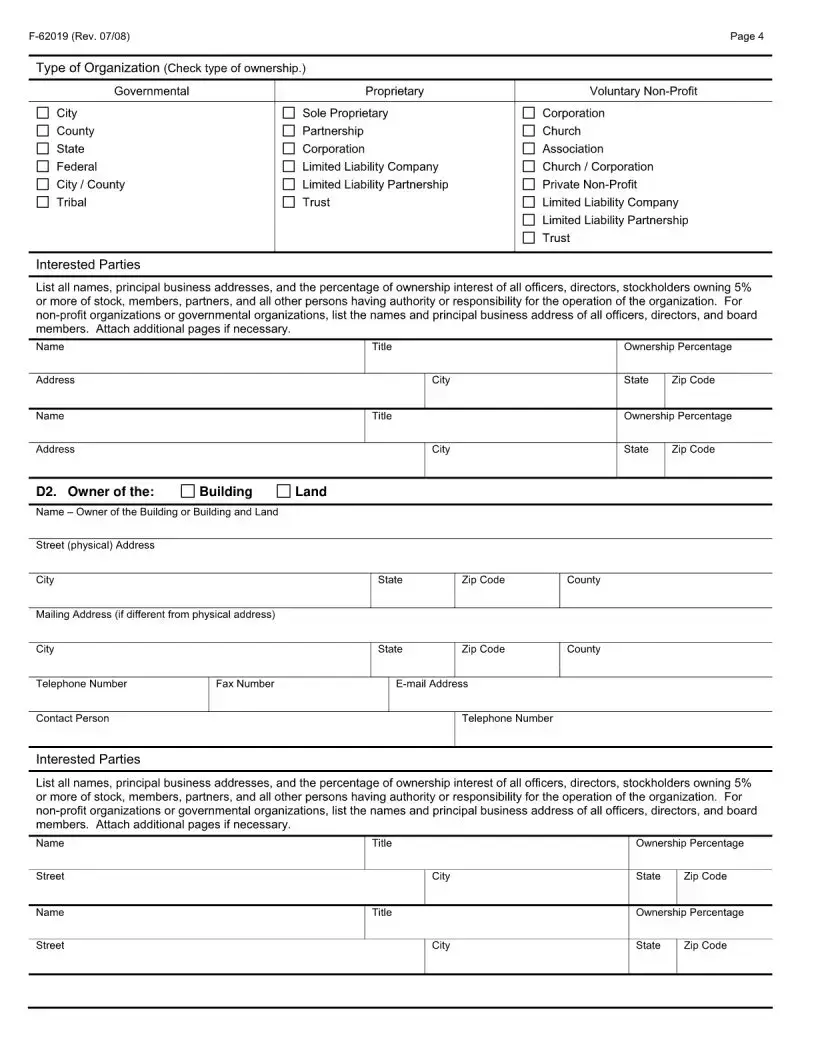
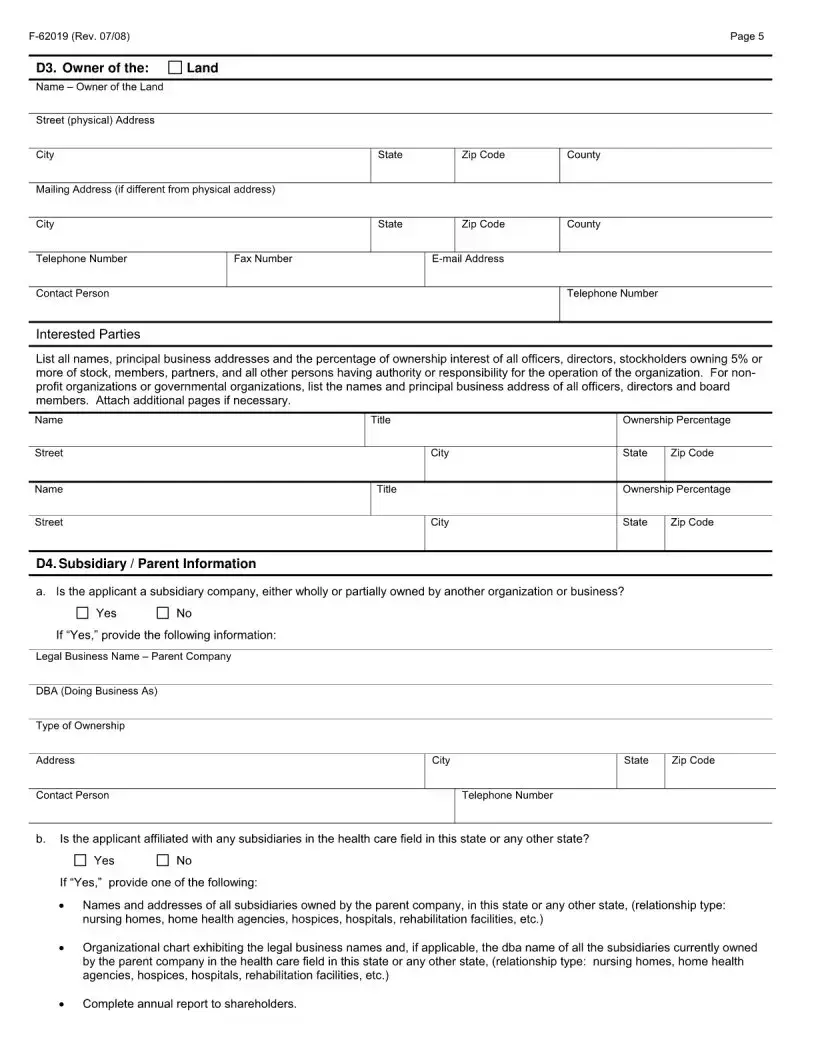
| Ownership Details | Applicants must provide information about the ownership structure, including names and addresses of all interested parties. |
| Contact Information | Contact information for the facility, including telephone and email addresses, is required for communication purposes. |
Popular PDF Forms
Wisconsin Cfs 2114 - The form requires details such as the employee's name, the title and author of the material read, or the presenter and length of the video watched.
The IRS W-9 form is a tax document used by individuals and businesses to provide their taxpayer identification number (TIN) to the person or entity requesting it. Completing this form is essential for reporting income and ensuring compliance with tax regulations. For those seeking assistance in filling out this form, resources like PDF Templates Online can be invaluable in avoiding potential issues with the IRS.
Wisconsin Uniform Building Permit Application - Emphasizes a procedural approach to obtaining necessary permits for building modifications or new construction endeavors.
Transfer Title Wisconsin - Form MV2185: The dealer's ally in facilitating vehicle demonstrations under Wisconsin law.